
- June 17, 2019
-
 Clayton Clews
Clayton Clews - Uncategorized

Podiatric Medicine: Office Surgical Procedures and Local Anaesthesia Techniques
In this blog, I will discuss office surgical procedures and local anaesthesia techniques I commonly utilise in my private practice rooms. These surgical techniques usually permanently resolve the patient’s foot complaint. Local anaesthesia techniques, with and without cortisone, reduce/eliminate pain and can be used in addition to other types of treatment to maximise patient outcomes. Part One of this blog will focus on ‘In-growing Toe Nail Surgery’, which has a success rate of over 95% in eliminating painful in-growing toe nails.
PART ONE: In-growing Toe Nail Surgery
An ingrowing toe nail is a common affliction across the spectrum of age groups. That is, it is common in children and teenagers but can also afflict the elderly. The most common toe affected with this condition is the 1st, although it can affect the nails of the 2nd, 3rd and 4th toes. A 5th in-growing toe nail is rare. Problems involving the 5th toe are commonly associated with a hard corn growing into the base and side of the nail (onychoclavus) or a soft corn present between the 4th and 5th toes (heloma molle) or a hard corn directly on top of the 5th toe.
The most common cause of an ingrowing toe nail is excessive curvature of the nail (called transverse (side to side) curvature or involution of the nail). This causes the nail to ‘dig into the sides’ of the affected toe. The side of the toe is commonly inflamed, can become infected and is often very painful to touch. It is not uncommon for excess tissue, called hypergranulation tissue, to form over the edge of the nail. In some cases, if both sides of it are involved, hypergranulation tissue can almost cover the entire nail.
Figures 1 and 2 demonstrate a typical in-growing toe nail.

Nail surgery is reserved for cases where non-surgical measures don’t provide the patient with a satisfactory outcome or do not definitively resolve their concern. It is common for ingrowing toe nails to recur and be problematic for years. Some patients are satisfied to have their complaint treated from time-to-time, whilst others wish to have a permanent fix for their problem and it is at this time when surgery becomes a viable option.
1.1 Nail Avulsion and Cautery Procedure
This is an excellent in room procedure, which provides a reliable and permanent solution to ingrowing toenails. The incidence of recurrence is extremely low.
This is a technique where a wedge of nail is removed from the afflicted side of the involved toe. Sometimes only one side needs to have a wedge of nail removed, whilst at other times four or more sides need to be removed, especially when both 1st toes nails are in-growing. Even the 2nd, 3rd and 4th toe nails can grow in, although it is rare for the 5th toe to be afflicted with this complaint. Issues associated with the 5th toe, are usually associated with a corn at the base of the nail (an onychoclavus), a hard corn on top of the toe or a soft corn between the 4th and 5th toes.
Avulsing the offending nail section is only part of the surgical procedure. The ‘cautery component’, using an agent such as 80% phenol is important to achieve a permanent result. The phenol cauterises/sterilises the matrix (nail growth tissue) to prevent future growth of the section of nail, which has been removed.
Figure 3 – This shows a simple sequence of the nail avulsion and cautery procedure. The affected side of the toe nail is first elevated (A), incised and removed (B and C) and then cauterised typically with liquid phenol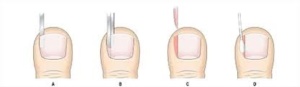
Surgery is performed after the administration of a local anaesthetic and following the application of a tourniquet to the toe. With these techniques, the procedure should be painless (following the injection) and minimal blood should be present, although some bleeding will always be evident. Usually there is minimal post-operative pain, but if there is some, this can be managed with oral analgesic/anti-inflammatory medications.
In some cases, a total nail avulsion with cautery will need to be performed. This is usually associated with symptomatic thickened or deformed nails, which have not responded to non- surgical forms of treatment. Interestingly, the total removal of a deformed/thickened nail results in a better appearance to the toe, in comparison to leaving the nail in place. A total nail avulsion and cautery procedure usually takes slightly longer to heal than the partial nail avulsion technique. Partial nail avulsion with cautery procedure usually take between 4-6 weeks to fully heal, with 70-80% of healing competed in about 2-weeks. I advise salt foot baths, the application of a topical antiseptic and a protective toe cover whilst healing is occurring. This type of healing is referred to secondary intention healing, whilst that involving stitches (sutures), which is not necessary for this technique, is termed primary intention healing.
Figure 4 Figure 5


Figure 4 demonstrates full healing following a partial nail avulsion with cautery procedure, whilst Figure 5 demonstrates full healing following a total nail avulsion with cautery procedure. Contrary to what may be believed, the total removal of the nail results in an acceptable cosmetic appearance.
In terms of complications, this technique is associated with very few. A recurrence of an in-growing toe nail is possible, and in the few instances where this has happened with me, I have performed a revision procedure free of charge. Post-operative infection can occur however, this can be dramatically reduced with proper after care. Of course, nail surgery of this type is performed using an aseptic technique, where gloves and instruments are fully sterilised. In some cases, anti-biotic therapy will need to be undertaken to eliminate the infective organisms. A script for an antibiotic can be provided to address this. Infection is more common in the diabetic and peripheral vascular disease patients but can occur in anyone, should the circumstances be suitable.
1.2 Sharps Procedures
Whilst such procedures can be performed in my rooms, I usually reserve them for a hospital setting. Sharps procedures involve the use of a scalpel blade to dissect away (or excise) the offending nail and surrounding soft tissue, including the matrix tissue to ensure there is no future growth of the offending nail or nail section.
Two common procedures are the Zadik’s technique (used to remove the entire nail) and the Winograd procedure (used to remove the side of each offending nail – Figures 6-10). The Winograd procedure is similar to the nail avulsion and cautery procedure, except that the nail and soft tissue including matrix are removed using a scalpel blade. Removal of the matrix tissue is termed a matrixectomy procedure. The Winograd procedure is an excellent technique to revise failed nail surgeries (Figure 11), address severe chronic in-growing toe nails, where there is a great deal of hypergranulation tissue and for debulking the nail fold (where the side of the nail sits) when it is excessively bulbous or enlarged.
Figure 6 (Before surgery) Figure 7


Figure 8 & 9


Figure 10

Figures 6 -10 demonstrate how an in-growing toe nail (Figure 6) has been surgically excised using a Sharps procedure (Winograd technique). This involves removal of the offending nail piece and the tissue which grows this (the matrix), followed by repair of the wound with sutures. Figure 10 demonstrates the appearance of the toe following 2-weeks of healing. Note the application of Betadine antiseptic solution to the toe. This will be followed by a light dressing. The patient made a full recovery with a normal looking and painless toe.
Figure 11: Failed previous nail surgery by another surgeon. This patient would benefit from a revision procedure, either Winograd or Zadik’s.
