


Hallux Valgus (Bunions - progressive dislocation of the big toe joint)
This disorder is a progressive dislocation of the 1st metatarsophalangeal joint (big toe joint) and is primarily inherited. It is commonly associated with pain and osteoarthritis of this particular joint as well as progressive subluxation of the lesser metatarsophalangeal joints (small toe joints) leading to progressive hammer/claw toes and associated plantar (bottom of the forefoot) pain. Corn and callouses are common consequences of a foot afflicted with hallux valgus. Nerve entrapments (ie-neuromas) exhibit a high incidence in patients exhibited a hallux valgus deformity. Patients with hallux valgus often experience a reduction in quality of life, mobility and experience foot wear fitting difficulties.
Hallux valgus and its associated complaints can be treated in many cases without surgery depending upon the severity of the disorder. Primary foot care can be used to address corns and callouses and thickened/ingrowing toe nails associated with it. Foot orthoses can be used to reduce pressure to the foot and control foot pronation commonly associated with its development or progression. Shoes can be used to accommodate ‘bunions’ and reduce pressure from the top of the lesser toes. Medications can be a useful compliment to these measures.
Hallux valgus surgery is reported in the literature as highly reliable at treating this condition when other forms of treatment have proven ineffective or in more advanced cases where conservative care (ie – non-operative management) is not indicated. There are many types of potential procedures which can be performed and these options can be discussed with our practitioners.

Hallux valgus (bunions) usually worsen over time.
To see a graphic of hallux valgus surgery (video one) please click below.
Hallux Rigidus (Osteoarthritis of the big toe joint)
This disorder is a progressive osteoarthritic change, taking place at the 1st metatarsophalangeal joint. It has been associated with many possible causes. It can be post-traumatic (ie-secondary to injury) but it often isn’t. The rheumatoid arthritic and diabetic patient are more prone to developing this condition but it has a broad based prevalence. As with hallux valgus patients with hallux rigidus often experience a reduction in quality of life, mobility and experience foot wear fitting difficulties.
Hallux rigidus can be managed quite well in the early stages with foot orthoses and appropriate footwear. However, once the range of motion reduces significantly then conservative management (ie-non-surgical) proves far less effective. The extent of damage can be assessed by plain film radiograph evaluation (x-rays), range of motion studies and the use of quality of life measurement tools such as the Foot Health Status Questionnaire. As with hallux valgus surgery a large variety of techniques exist to address the pain and disability associated with this complaint. Such technique may preserve the joint, reconstruct the joint or be joint destructive. Each of these options can be discussed with the appropriate procedure selected based on the extent of the joint disease process and preference of the patient.
A technique called a capsular interpositional arthroplasty procedure is commonly used by podiatric surgeons preserving as much range of motion as possible whilst eliminating pain. An arthrodesis procedure (ie- joint fusion with or without a graft - video three) is reported by the literature as achieving excellent reduction in pain but it completely eliminated range of motion of the joint. This may not be a preference for some patients and should be discussed with our practitioners.
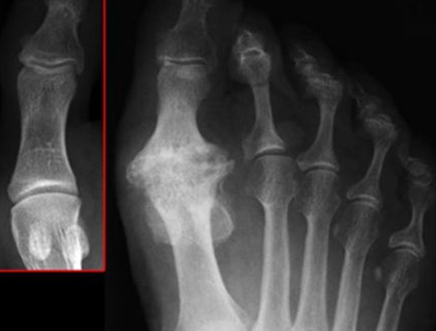
This plain film radiograph (x-ray) demonstrates a normal joint in comparison with a severe case of hallux rigidus.
An arthrodesis procedure with/without a bone graft can be an effective means of treating hallux rigidis. Please click below (video two) to see a simple example of this procedure.
Hammer/Claw Toes
These may occur in isolation or may affected multiple toes involving both feet (see below picture). People afflicted with claw toes commonly experience corns and callouses to the tips and dorsum (top) of the toes and to the plantar (bottom) of the forefoot. In severe cases the fat pad which protects the joints of the plantar forefoot (lesser metatarsophalangeal joints) is displaced distally (ie- shift towards to toes and off the joints) leaving them exposed and painful. Patient with rheumatoid arthritis and diabetes have a higher incidence of claw/hammer toes.
Hammer toes can be treated in many cases without surgery depending upon the severity of the complaint. Primary foot care can be used to address corns and callouses and thickened/ingrowing toe nails associated with hammer/claw toes. Foot orthoses can be used to reduce pressure to the plantar forefoot (ball of the foot). This pressure is commonly associated with hammer/claw toe formation often caused by an acute or progressive tear of the plantar plate. Shoes can be used to accommodate hammer/claw toes and reduce pressure from the top of the lesser toes. Medications can be a useful compliment to these measures.
Surgery can be used to straighten toes, eliminate corns and callous associated with them and reduce pain. The straightening of toes is important in the diabetic and rheumatoid patient as they will be more susceptible to infection because of localised tissue trauma and potential ulceration. Once the protective layer of skin is breached a portal of entry is provided to bacteria leading cellulitis (soft tissue infection) and/or osteomyelitis (bone infection).
Digital surgery (corrective toe surgery) is complex and many techniques exist to straighten toes. Such techniques can be discussed with our practitioners.

Hammer toes are commonly caused by progressive or acute rupture of the plantar plate (video three). There are a number of surgical methods used to correct claw/hammer toe deformities (video four). Please click below to see an explanation of the plantar plate rupture and to see a simple example of a hammer toe corrective procedure.